
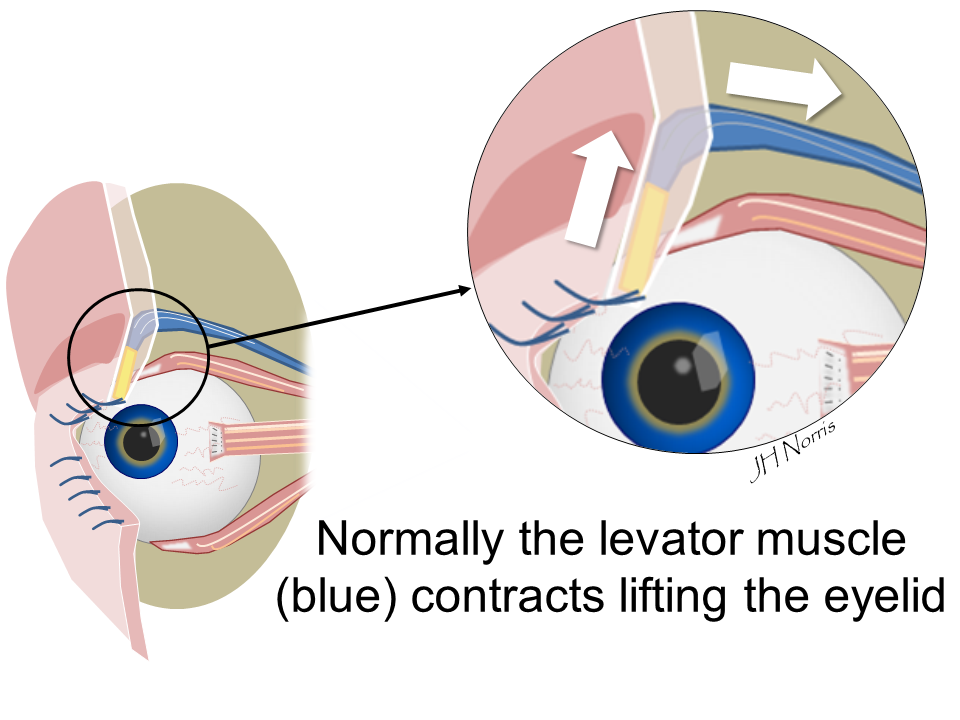
The muscle in the eyelid that lifts the eyelid is called the ‘levator muscle’ (Tap image below to enlarge). When the levator muscle contracts the eyelid lifts.
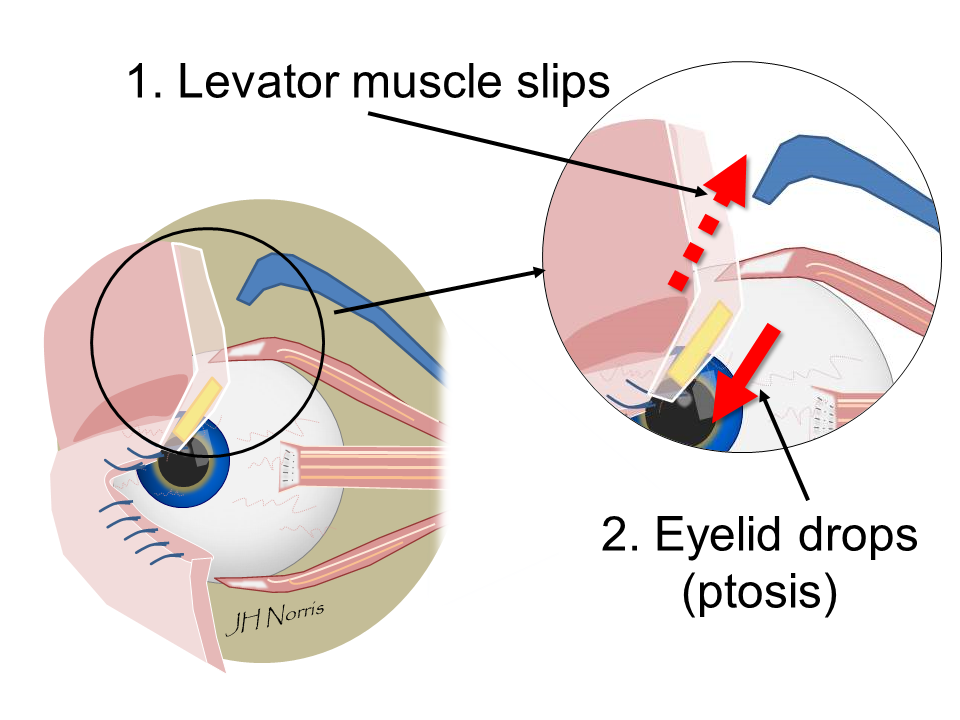
In ptosis the muscle can slip from its insertion into the eyelid and the eyelid drops (Tap image to enlarge).
The mainstay of treatment is surgery which is aimed at correcting the position of the eyelid.
We normally perform your surgery under local anaesthetic which is given in the operating room. Occasionally we can give sedation at the same time if you are uncomfortable about having a local anaesthetic on its own.
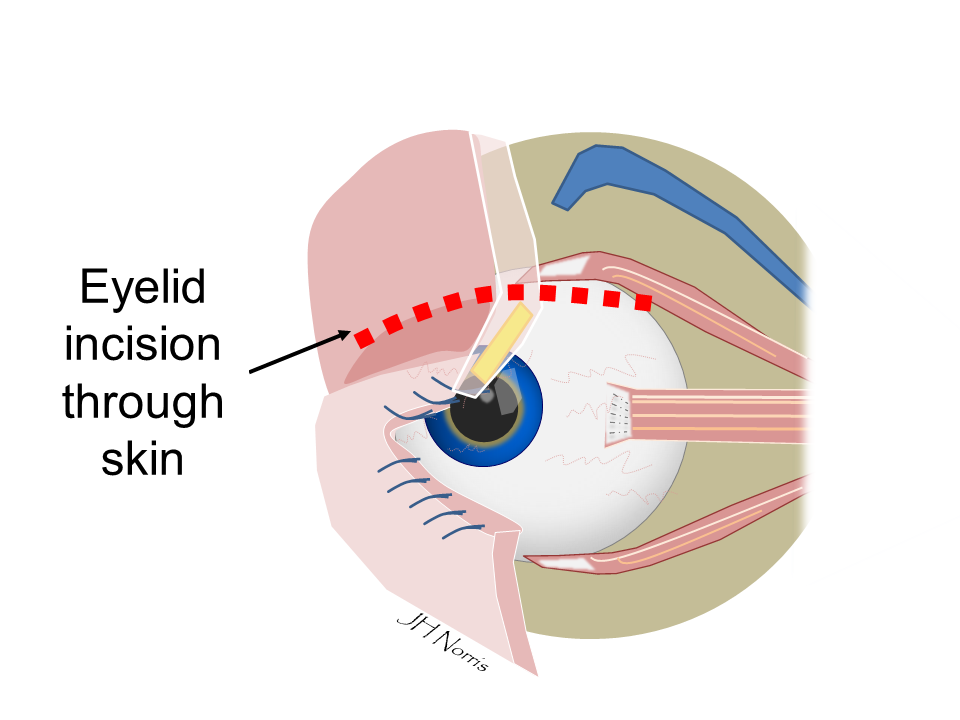
There are essentially two options for lifting the eyelid: (i) via a skin incision (anterior approach) or (ii) through a hidden incision underneath the eyelid (posterior approach). Mr Norris is trained in both techniques and can discuss these with you.
ANTERIOR (SKIN) APPROACH
In some cases the incision is made on the front surface of the eyelid whereby Mr Norris may also remove some of the excess upper eyelid skin (dermatochalasis – see information). This second procedure is known as a blepharoplasty procedure. The surgery normally takes about 25 minutes per eyelid but can sometimes take longer. The scar heals within the skin crease.
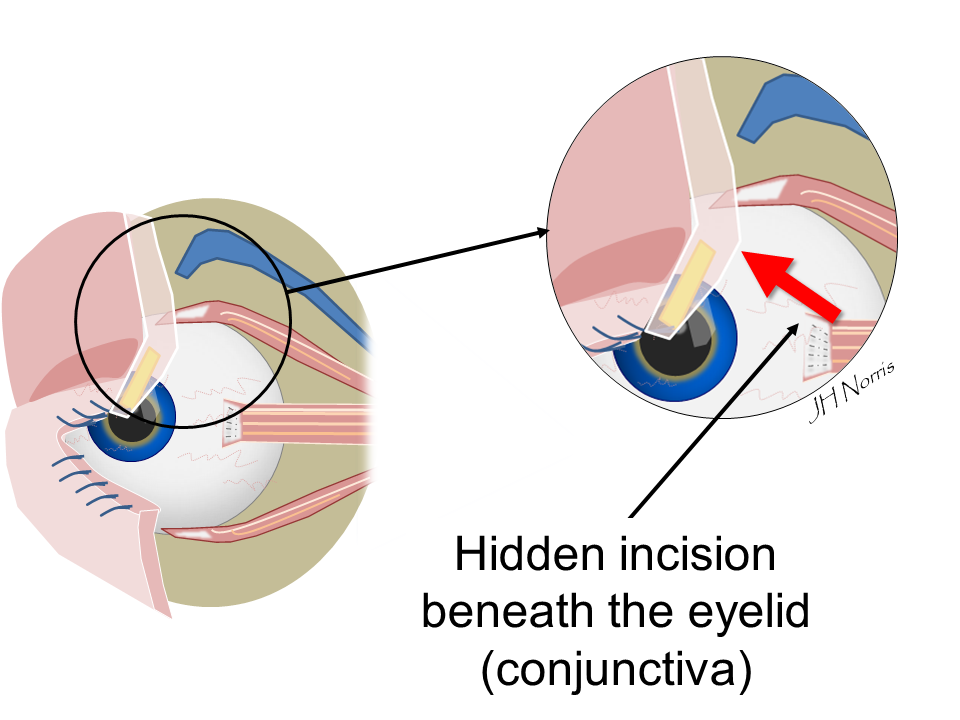
POSTERIOR APPROACH
This technique does not leave a linear scar on the skin but onkly two small sutures. This technique is not suitable for all types of ptosis correction but can be very effective. The incision is made through the back of the eyelid via a layer of tissue known as conjunctiva.
The risks of surgery include postoperative bleeding, scarring to the eyelids, dry eye and infection. We advise that you use an antibiotic ointment after the surgery (see below) to help reduce the risk of infection.
Occasionally we may under or over correct the position of the eyelid. Most of these complications can be corrected if required with a second operation.
The most serious risk of any eyelid surgery performed is damage to your eyesight. Fortunately this risk is extremely rare.
On the day of surgery you will be told a time and place to come in to the hospital. You will be met by the nursing team and one of the surgical team will also see you.
If you are for day case surgery you will need to make sure that someone can be with you on the evening of surgery. If you are coming to stay the night you will need to bring some overnight clothes and toiletries for the duration of you stay. We advise that you also bring in your medications with you when you come into hospital.
This type of surgery is usually performed as a day case operation and we normally allow you to go home about 30-60 minutes after you surgery is finished.
The eyelids will be bruised after surgery and you may have some blood stained tears which is quite normal initially.
The eyelid will often look a little swollen for the first couple of weeks. In addition you may find it difficult to fully close th eyes over the first couple of days. This settles down as the eyelid relaxes into its normal position.
We usually see you 1-2 weeks after surgery to remove any sutures.
Normally we ask that you keep the wounds around your eye clean after surgery. You can clean the wound by allowing boiled water to cool and gently dabbing the wounds with a cotton bud.
We will give you some antibiotic ointment (usually Chloramphenicol) to apply to the wounds and to the eyes after the surgery to help protect against infection and to help lubricate the eyes for two weeks.
We normally advise that you apply ice compresses to the eyelids after surgery for three times a day for 5 minutes each time. This is to help reduce the bruising.
We will see you 1-2 weeks after surgery to remove any sutures.
You should avoid any strenuous activity including lifting heavy objects for at least two weeks and avoid swimming for three weeks after surgery.
Usually patients are quite anxious after having surgery near their eyes and most problems do settle with time. Problems that require immediate attention are the onset of new double vision, loss of vision and pain that cannot be controlled with regular painkillers.
Please refer to the emergency contact page (in contacts) if you need advice.
Author: Mr Jonathan Norris FRCOphth